In 2013 I moved to Ndola, a city in northern Zambia, to work on an HIV research project. Ndola is the hub of the country’s copper mining industry, a bustling commercial center that draws entrepreneurs from South Africa and beyond. My organization worked with government clinics in villages around the Ndola area to provide HIV and family-planning counseling, care, and education. I’d recently graduated from a master’s program in public health, and a US-based research organization had hired me to co-lead a year-long study of HIV infection among women.
Dr. Martin Luther King delivering his "I Have a Dream" speech in Washington on August 28, 1963. National Archives and Records Administration, via Wikimedia
Dr. Martin Luther King delivering his “I Have a Dream” speech in Washington on August 28, 1963. National Archives and Records Administration, via Wikimedia
All the discussions today of how much racial progress we’ve made since Dr. Martin Luther King was alive reminded me of a disturbing point about the black−white health gap mentioned in recent research, some of which I discussed in an Atlanticessay over the weekend.
According to the Centers for Disease Control, African Americans have been catching up with whites in terms of life expectancy at birth. So things are looking up, right?
Yes, and no. To a sizeable extent, what explains the narrowing of the life-expectancy gap in the last couple decades is not just that things are better for African Americans (though they have improved), but also that things are worse for whites—working-class whites above all.
A New York Timespiece over the weekend highlighted this fact. “A once yawning gap between death rates for blacks and whites has shrunk by two-thirds”—but that’s not because both groups are doing better, according to the article. Overall mortality has declined for African Americans of all ages, but it has risen for most whites (specifically, all groups except men and women ages 54-64 and men ages 35-44).
Furthermore, younger whites (ages 25-34) have seen the largest upticks in deaths, largely because of soaring rates of drug overdoses, and those who have little education are dying at the highest rates. The mortality rate has dropped for younger African Americans, a decline apparently driven by lower rates of death from AIDS. Together these trends have cut the demographic distance between the two groups substantially.
For middle-age African Americans, the progress in improving health outcomes implied by the shrinking black−white mortality gap is also less cause for celebration than it might seem at first.
A much-discussed study last year by the economists Anne Case* and Angus Deaton found that huge spikes in deaths by suicide and drug poisonings over the last couple decades have meant that the trend of declining mortality rates we’ve seen for generations actually reversed for whites ages 45-54 between 1999 and 2013. Again, those with little education were hit the hardest.
In my Atlanticpiece, I pointed out that the growing social isolation and economic insecurity of the white working class might explain some of these trends. One of the caveats I mentioned is that death and disease rates remain much higher among African Americans and Latinos. (I should have been more precise in the article: although Latinos have higher rates of chronic liver disease, diabetes, obesity, and poorly controlled high blood pressure, they have lower rates of cancer and heart disease, and lower or at least equivalentrates of death).
But it’s not just that the black−white gap persists. Here’s an important passage from Case and Deaton’s paper:
Over the 15-[year] period, midlife all-cause mortality fell by more than 200 per 100,000 for black non-Hispanics, and by more than 60 per 100,000 for Hispanics. By contrast, white non-Hispanic mortality rose by 34 per 100,000. CDC reports have highlighted the narrowing of the black−white gap in life expectancy. However, for ages 45–54, the narrowing of the mortality rate ratio in this period [1999−2013] was largely driven by increased white mortality; if white non-Hispanic mortality had continued to decline at 1.8% per year, the ratio in 2013 would have been 1.97. The role played by changing white mortality rates in the narrowing of the black−white life expectancy gap (2003−2008) has been previously noted. It is far from clear that progress in black longevity should be benchmarked against US whites.
Let me reiterate their point: for Americans ages 45-54, the narrowing in the black−white gap in life expectancy in recent decades was “largely driven” by more deaths among whites.
It’s heartening that overall life expectancy is increasing for many Americans, including African Americans. But it’s also important to remember that, almost a half century after King’s death, people of all races continue to be left out of this country’s progress, and some—whites and nonwhites—may, in fact, be seeing an unprecedented step backward.
* I want to apologize to Dr. Anne Case for mistakenly identifying her as “Susan Case” in the original version of my article in the Atlantic. (The only reason I can think of for why I made that dumb mistake is that a friend of mine is named Susan Caisse.) This brilliant scholar has already suffered the injustice of having her study erroneously called the “Deaton and Case study” rather than the “Case and Deaton study” (for better or worse, first authorship is everything to us academics), and here I’ve added insult to indignity. My sincere apologies.
I had no friend quite like Ed. We also hated each other.
He was with me all the time. He knew all my secrets. When I was in high school, all I wanted was to be perfect. At 5:30 a.m. I would run six miles. Then, after school, I would study until 10 p.m., breaking only for dinner. I always had to get an A. He understood why I would wrap my hips and abdomen in duct tape to keep it all in, so that my tight pants would fit perfectly and no amount of fat could bubble over the top.
When we had meals together, he would reassure me that it was okay to eat only fruits and vegetables. He would agree when I would say, “I’m fat, I need to lose weight.” He saw what I saw in the mirror.
He didn’t mind that I didn’t make much of an effort to get to know him. He understood that I was wrapped up in my own troubles.
I came home from college for winter break, and my parents said I had lost too much weight. They wanted to know what was happening. I lied. I told them I was fine, just busy. Ed and I laughed about it later.
When I returned to school after a Christmas spent eating only cranberries, frozen fruit, and broccoli, I went to a dietician. She told me that I was sick and needed to gain weight. I said I would try. Ed and I walked home from the appointment. “Great job,” he told me. We made fun of her stupid meal plan and her naïveté in believing me. I repeated the lie to my parents, too.
But after several months, my body broke down. My doctor told me that I couldn’t physically exert myself in any way, lest I have a heart attack. The news didn’t faze Ed. He smiled and said, “Let’s go for a run. You’re looking a little heavy.”
“Ed,” I said, “I really don’t think I can run.”
I agreed to go into outpatient treatment. Ever the loyal friend, Ed came with me. “These other girls are sicker than you,” he said. “You don’t belong here.” I looked around the room. Some had tubes in their noses. Others were drinking protein shakes because they had refused lunch. Ed and I laughed at these pitiful creatures. We thought up ways I could outsmart the staff. “Exercise when you get home at night,” he told me as we sat in the waiting room. “Don’t pay attention during the activities.”
I did what he said. I had entered treatment in June, but a month later, I still hadn’t gained any weight. I was told I would need to receive inpatient treatment and defer school for a semester.
That’s when I turned my back on Ed. I still liked how I looked at seventy-five pounds. But what would it matter if I were cooped up in a treatment facility, isolated from everyone I knew, living among ghosts? I started to realize that I might become like the people around me: pale, emotionless, wheelchair-bound—barely able to move a muscle.
I began seeing a therapist. She told me I needed to get Ed out of my life. “Tell him ‘No,’” she said. “Every time you sit down to a meal, every time you want to run six miles, don’t do what he’s telling you to do. It will get easier each time. Trust me.”
I did trust her. She became a new friend, and with time I learned to listen to her instead of Ed.
It took about a year to get myself over 100 pounds and regain the trust of my parents after promising them repeatedly that I would try to get better.
Ed never stopped hectoring me. On my wedding day, he told me my dress didn’t fit properly. When I thought about having kids, Ed warned that I would gain too much weight and turn ugly.
But by then I had found a true best friend, my husband. He told me he loved how I looked in my wedding dress. Later, we decided to have children.
In the seven years since I had my falling out with Ed, I’ve learned to tune out diet fads, step away from the mirror, and divert myself from self-destructive thinking.
Ed, my eating disorder, is still around. He never does go away for good, I’ve learned. Sometimes he joins me during meals or exercise. But it’s not the same as it was. He and I aren’t friends anymore.
Best of In The Fray 2014. Once thought cured by modern medicine, tuberculosis is making a global comeback. Rampant misuse of antibiotics and broken health-care systems have spawned deadly, drug-resistant strains that are now present in virtually every country.
By Octavio Raygoza
Mycobacterium tuberculosis, the pathogen that causes TB. NIAID
She looks like a child: a baby face and large, round eyes, long and thin arms that make her seem gawky. When she sees me, her eyes brighten, and she struggles to sit up in her hospital bed. The blanket covering her drops, revealing a frail and gaunt body—a nineteen-year-old’s body. Five feet, four inches, she weighs only eighty pounds.
Sonam Yambhare is dying, and there is little modern medicine can do for her. Two years ago, she contracted a drug-resistant form of tuberculosis in her lungs. The bacteria that cause the disease have destroyed her macrophages, the body’s first defenders against foreign invasion. Constant nausea, loss of appetite, and vomiting—symptoms of the disease—have emaciated her. All medications have been infective. In her weakened state, another serious infection will likely kill her.
Ward Number Eight of the Sewri Tuberculosis Hospital is a silent room with gray concrete walls. It is a world away from the chaotic streets of Mumbai. And it is a world away from the rest of Indian society. With nowhere else to go, neglected and stigmatized TB patients like Yambhare come here—even from towns and villages hundreds of miles away—to wait out the last stages of the disease, sometimes alone.
“Everyone is depressed here,” says Chandge Mokshada, a young doctor on her rounds. In the crumbling ward, dozens of women lay quietly on their beds. There is little chance they will recover, Mokshada says. “We mostly lose our patients.”
One of the world’s most lethal infectious diseases is making a comeback. Two centuries ago, tuberculosis was responsible for a quarter of all deaths in parts of Europe and the US. Known as the “white plague” or “white death” due to the way it blanched the skin, the disease left a deep imprint on the culture. Thomas Mann and Fyodor Dostoevsky wrote about it. Emily Brontë and Henry David Thoreau died from it.
After the development of effective antibiotics in the 1940s, deaths from tuberculosis plummeted. But TB remains a formidable killer in many parts of the world. And in recent years, it has evolved in frightening ways. Its virulent new strains now defy many or all known antibiotics. And while they have ravaged Asian countries in particular, these deadlier forms of the disease are spreading everywhere.
Last month, the World Health Organization released a report about the surge in infectious diseases that are fast becoming untreatable. “A post-antibiotic era—in which common infections and minor injuries can kill—is a very real possibility for the 21st century,“ the report read. The WHO singled out drug-resistant tuberculosis as one of the greatest dangers. In 2012, it accounted for 450,000 new cases and 170,000 deaths—that is, less than 4 percent of those newly infected with TB, but 13 percent of those the disease killed. The total number of confirmed cases has grown sevenfold over seven years, with India, China, and Russia accounting for more than half of new infections. (The official statistics also understate the size of the problem, since many of the hardest-hit countries report bogus numbers.)
New strains of TB arise when the old ones are not properly treated. Not taking a full course of antibiotics, for example, can merely weaken, rather than eradicate, the bacteria that cause the disease. The remaining bacteria evolve to adapt to the drug, turning a treatable strain of TB into a resistant one.
The problem has gotten progressively worse. At one point, health officials believed TB could be eliminated. But in the 1980s, tuberculosis strains emerged that resisted the most common and safe anti-TB drugs. In the past decade, even second-line treatments have become ineffective against certain tough strains that fall under the category of “extensively drug-resistant tuberculosis” (about 10 percent of drug-resistant TB cases). To deal with them, doctors will put patients on more than one of these toxic drugs. Their side effects, however, can be severe, ranging from acne, weight loss, and skin discoloration to hepatitis, depression, and hallucinations.
For the hardest-to-treat strains, doctors are now forced to use so-called third-line drugs, an even more toxic regimen whose effects have yet to be fully tested.
Today, resistant strains can be found virtually everywhere, including the United States and Europe. But perhaps nowhere is the crisis more real than in India. The world’s second most populous country has a quarter of its TB cases—and now, many of the hardest ones to treat. While the number of Indians suffering from the disease has actually gone down in recent years, thanks in part to widespread vaccination, the WHO estimates that in 2012 the country had 21,000 new cases of drug-resistant TB of the lungs—an exponential increase from the few dozen cases the government had been reporting just six years earlier.
India also has the dubious distinction of being one of three countries—Iran and Italy being the others—where certain strains of TB have resisted every drug used against them. Four years ago, Zarir Udwadia, a noted pulmonologist at Mumbai’s Hinduja Hospital, identified twelve patients suffering from untreatable TB infections. (Three of the twelve have since died; the others have been taken into isolation by the government.) Udwadia and other researchers have described these kinds of cases as “totally drug-resistant.”
The Indian government disputes the categorization, arguing that these strains have not been tested against all of the experimental third-line drugs. Another term, “extremely drug-resistant TB,” gets around the worry of some experts that classifying such a common disease as untreatable may cause panic.
Regardless of what they are called, these hardy strains have the power to push societies back to a time before antibiotics, when the “white plague” was all but unstoppable. “If not contained,” says infectious disease specialist Charles Chiu of the University of California, San Francisco, “it poses a big problem to the world.”
In India, those infected with TB tend to be the most vulnerable people in society. Yambhare was born into a low caste. She lived in a cramped apartment, where she shared a room with her mother and two sisters. Every day she took overcrowded trains from her home in the countryside to Mumbai, where she helped her mother clean houses. In other words, her poverty made it far more likely that she would be exposed to TB, which often (though not always) settles in the lungs and can be transmitted through the air.
Two years ago, Yambhare developed a persistent cough. She visited one of the private medical clinics that line the teeming streets of the western suburb of Bandra. There, a doctor diagnosed her with tuberculosis, and Yambhare began taking antibiotics. When her family saw no improvement over two years, they switched doctors. The new doctor prescribed more drugs.
No one bothered to give her a drug-sensitivity test. The test would have revealed what strain of TB she had, and a competent doctor could have then prescribed the correct drug. Instead, the incomplete and inept treatment that Yambhare received gave the bacteria the chance to adapt and become stronger. It soon developed a resistance to all four of the first-line drugs used to treat TB.
In Yambhare’s case and thousands of others, a broken health-care system has made the problem of drug-resistant TB much worse. Hospitals are overcrowded, and the services provided are minimal. So Indians—rich and poor—flock to private doctors. But the slapdash treatment they tend to provide, with laxly administered drugs and inadequate follow-up care, has allowed drug-resistant TB to spread wildly.
Udwadia, the Mumbai pulmonologist, says that many of these doctors are unscrupulous, and most are uninformed. In 2010, he conducted a study in Mumbai’s Dharavi slum, one of Asia’s largest and the origin of many of the city’s most severe TB cases. He asked more than a hundred doctors in the area to “write a prescription for a common TB patient.” Only six were able to do it correctly. Half of the doctors he surveyed were practitioners of alternative therapies with no grounding in modern science.
Udwadia argues that India needs a law that will let only designated specialists treat drug-resistant tuberculosis patients. But at the moment the government does not bother keeping detailed records on the many private doctors now operating, much less ensuring they provide adequate care.
“The government has no control over private practitioners,” says an official in the health ministry, speaking on condition of anonymity since he is not authorized to talk to the media. “They require only once-in-a-lifetime registration, and there is no chance for them to lose their license.”
Calls for regulation by experts like Udwadia, the official says, are silenced, ridiculed, or ignored. Meanwhile, the government has been accused of underreporting the number of new cases of drug-resistant TB every year. In 2011 the official count was 4,200 cases; the next year, the government began adjusting its figures to resemble the WHO’s estimates, and the number of reported cases quadrupled. (Indian health ministry officials did not respond to emails asking for comment.)
In terms of its anti-TB spending, however, the government has been devoting more resources. In 2013 it budgeted $182 million to fight the epidemic.
Some of this money will go toward upgrading the 103-year-old Sewri hospital, which could use it. In its ward for drug-resistant patients, there is no medical equipment in sight; records are kept in rusted metal cabinets. The most pernicious forms of TB are hitting a health-care infrastructure poorly equipped to deal with them.
Every year, more than eight million people fall ill with tuberculosis. More than a million die from it, placing TB just a notch below AIDS in its globe-spanning lethality. And a whopping one-third of the world’s population has what is called “latent TB”: they are infected by the bacteria, and a tenth of them will go on to develop the disease at some point in their lifetimes. Drug-resistant TB, in other words, is just one part of a global health emergency.
Meanwhile, the problem goes ignored in rich countries. Antibiotic treatments for TB have been so successful there that most people’s experience with the disease today is limited to works of literature: novels and poems with archaic references to “consumption” and TB sanatoriums. But that may change someday soon. In the United States, a hundred new cases of drug-resistant TB are diagnosed every year, according to the Centers for Disease Control and Prevention. Cases of extensively drug-resistant TB have already been reported.
Paul Nunn, the WHO’s TB coordinator, says that these deadly strains have cropped up in certain European countries, too, though the reports have yet to be published. “If the health system of the world fails, the highly resistant strains will replace the old,” he adds. “We’ll see a worsening of the situation if nothing is done.” On the other hand, it may be only when the resistant strains become a major problem in rich countries that the profit-seeking pharmaceutical industry will take notice and pour real money into the development of potent new treatments.
Without effective drugs to combat the most resistant strains, doctors may have to revert to remedies from an earlier era. Udwadia recalls his first patient with untreatable TB. Twenty-six years old, she had spent the last five years trying a variety of anti-TB drugs, all of which had failed. As a last resort, she underwent a pneumonectomy, a high-risk medical procedure to remove a lung. The woman later died of complications from the surgery. The procedure had not been used on tuberculosis patients since the introduction of antibiotic treatments six decades ago.
Even though so many people are infected, TB still carries a terrible stigma in Indian culture. “People treat you with disgust,” Yambhare says. As she grew sicker, she became more isolated. Her sisters were told to stay away. Her friends stopped visiting. Finding a partner or even a job was impossible. She sunk into a depression.
Meanwhile, her family struggled to pay for her treatment. Their monthly household income was just $100—not uncommon in a country where one in three people lives on less than $1.25 a day. But the expensive second-line drugs cost $80 a month. And once she began taking them, the side effects kicked in. Her skin became discolored. Her muscles atrophied. Her weight dropped.
Eventually, Yambhare’s family could no longer care for her. They sent her to the Sewri hospital.
When I visit her in the ward, orderlies are carrying out the infected mattresses of previous patients. In a nearby courtyard, they set the mattresses afire.
Yambhare watches the smoke curl past the window near her bed. Below her, in the courtyard, stray dogs fight over bones.
Yambhare turns to me, an eerie shine in her eyes. “I don’t want to die,” she says through her mask. “I want to go home and help mother.”
Octavio Raygoza is a video journalist who covers sports, news, and culture. Twitter: @olraygoza
Dear Reader,In The Fray is a nonprofit staffed by volunteers. If you liked this piece, could you please donate $10? If you want to help, you can also:
At the heart of Sister, Brenda Davis’s documentary debut, are three inspiring stories of an Ethiopian health officer, a midwife in rural Cambodia, and a traditional birth attendant in Haiti. When Davis met Goitom Berhane in Ethiopia in 2008, she was taken with his vivacious personality and dedication to solving the maternal health crisis in his country. Berhane’s example encouraged Davis to explore women’s health as an international human rights issue. Eventually, he became a central figure in her film.
We meet Madame Bwa in the poverty-stricken Shada neighborhood of Cap-Haitien, Haiti. An aged woman who struggles with basic survival, Madame Bwa has delivered more than 12,000 children with no formal medical training.
In an area of Cambodia that is littered with land mines, Pum Mach puts her own life at risk so that geographically isolated mothers and their children may live through the common event of childbirth. In one of the more ghastly moments of Sister, a nineteen-year-old girl delivers her baby by caesarean section thanks to Mach identifying the child as breech and securing transportation to the nearest hospital, which is several hours away.
These moments make Sister as beautiful as it is brutal. The film showcases the passion of health workers who overcome incredibly difficult circumstances to combat the alarming rate of maternal and newborn deaths occurring around the globe — deaths that, with adequate care, are almost entirely preventable.
In The Fray spoke with Davis about her family’s experience with child mortality and the challenges of filming a tragic topic.
When did you develop an interest in maternal and child mortality?
My grandmother gave birth to sixteen children in rural Nova Scotia. Four died during childbirth and one died at the age of two. She lost her first child when she was nineteen and her last at thirty-nine. I remember my cousins coming together to buy a gravestone for all the children my grandma lost. They spoke about it casually because this happened a lot where my grandmother lived, but it had a lasting impact on me.
Why did you choose to explore this topic for your film?
As an artist, I’m interested in storytelling. If a subject is compelling to me, I want to pursue it, but I don’t want to speak for people. I want them to tell their own stories.
I was very fortunate to find people willing to tell their stories in Ethiopia, Cambodia, and Haiti. We were able to show similarities in women’s experiences, despite entirely different cultures, while also focusing on local strategies. The unifying theme to every story is a lack of access — access to basic health care, access to emergency obstetric care, and access to family planning.
How are health workers attempting to close these gaps in access?
It’s difficult to articulate just how important health workers are, and in many instances, it goes beyond the service they’re providing. In Ethiopia, Hirity Belay is a young woman who walks to places where there are no roads to provide women with the care they need to have healthy babies. While that service is invaluable, you must also consider what an amazing example she’s setting in these small villages. One of the things that inspired the name of the documentary was Hirity’s relationships. The women would often call each other “sister.” I thought this was so beautiful and warm.
Madam Bwa, a traditional birth attendant in Shada, Haiti.
In the case of Madame Bwa, being a traditional birth attendant has been passed down through her family. The work she does is important to her community, and for the most part Madame Bwa lives off donations from the families she helps. Traditional birth attendants fill a gap where there is nothing. I’m not a medical professional, but I don’t understand why so many people want to eliminate traditional birth attendants. They’re making a difference, and with a bit more support, they could be making a much bigger impact.
I found many of the scenes hard to watch, not because they’re graphic, but because they are heartbreaking. How do you approach filming people’s intimate tragedies respectfully?
In Ethiopia, we spent time in the hospital without cameras and became a familiar presence. The women often didn’t understand why we were filming or why anyone would be interested. I’d explain that we wanted to show what was going on in their communities.
Sister was definitely difficult to film, and the director of photography and I constantly struggled with the fear that we may be invading a woman’s privacy. When you’re meeting people in such intense and difficult circumstances, you constantly grapple with whether or not you’re being sensitive and respectful.
In some respects, I feel like Sister is a war movie. Women everywhere — but especially in developing countries — are fighting for their lives. What you see was exactly what was happening. The women, health workers, midwives, and birth attendants all speak for themselves and tell their own stories. It was a conscious decision not to narrate or pretend to know the answers.
What do you hope viewers take from the film?
I hope Sister encourages people to think critically about what the United States does that affects other countries — from a its inability to grow food to being littered with land mines. People should think about how they’re connected to what’s happening in other places, or how they’re complicit in it. Donating funds is awesome, but it’s not enough.
After her mother's unexplained death, a young woman ponders the long-term toll of not having access to adequate health care. A toothache brings on psychic hysteria about whether her own eventual demise will align with that of her mom.
I don’t know why my mom died at the age of forty-nine because my father refused to allow an autopsy. His superstitious and deeply traditional beliefs mean I’ll never know the cause of my mother’s death. Was it a complication from having high blood pressure? Did she have a heart attack? At this point, all I can do is speculate — so I do.
A theory I’ve come up with recently is that her death may have been caused by problems with her teeth. When my mom was in her thirties, her teeth began falling out for some unknown reason. By the time she died, she had only a few left in her mouth. I wonder if the pain and swelling in her face before she died was due to an untreated tooth abscess. A recent study shows that oral infections are causing more hospitalizations, and if left untreated, a tooth abscess can be deadly when bacteria spread.
“When money and access are not problems, an abscessed tooth can easily be treated with a root canal or an extraction,” reports the New York Times. “But increasingly, Americans rely on hospital emergency rooms for dental care, instead of regular dentist visits — a trend exacerbated by a lack of insurance coverage and trouble paying out of pocket.”
I remember times when I was growing up that my family used old newspapers instead of bathroom tissue because my parents couldn’t afford toilet paper. Having narrowly escaped homelessness, my father solicitously cut the newspaper into squares, and we laughed at the extent of his effort because that somehow made it less dispiriting. Some days we had electricity, and some days we didn’t. But the presence of stressed out, overworked parents was ubiquitous.
My tale of ill-fitting, hand-me-down, thrift-store clothes and sharing a bedroom with my older brothers is not unique. Anyone who grew up poor can tell you similar stories of the challenges that come from not having what you need, materially and emotionally. They can also tell you what it’s like to make decisions about their lives without the assumption of ever achieving financial security. It never occurred to me that I could have a life that didn’t involve economic struggle, and I wonder if my decision to become a writer isn’t a result of this. Who would seek out a lifetime of poverty other than someone for whom it was a prophecy?
Being a writer means I have no health insurance, no steady paycheck, and no stability. While writers who aspire to upward mobility say they’re simply “low income,” as though the condition is temporary, my intimate familiarity with life below the line of poverty makes me uninterested in feigning comfort through euphemistic niceties. It’s not comfortable juggling deadlines for a dozen publications while not technically being employed by any one. I thought I had accepted my lot, but a few weeks ago I began having problems with my teeth.
The dull ache persisted for days. Overwhelmed by my circumstance, I immediately assumed the worst. This was the beginning of the end. In two years, I’ll be thirty, and my teeth will start falling out. Soon after, I will die penniless and alone just like my mom.
I know this line of thinking probably seems extreme. A toothache doesn’t typically bring on psychic hysteria about one’s impending death, but if my life has taught me anything, it is that every misstep can be the start of a downward spiral. One illness can be the difference between making do and ruin.
For months I’ve been putting together a referral binder for a women’s recovery center where I am a volunteer. As soon as my tooth began to ache, I poured through the dental resources, frantically calling each practice to beg for an appointment. They all said the same thing: our budget has been slashed, and we are unable to accept new patients at this time.
One clinic told me their wait-list is over a year long. Another said my only option was to show up at 6 a.m. because the only way I would be seen is if I were one of the first three people in line, although that was only for extractions. All the receptionists I spoke with were deeply apologetic, and I could hear the sadness in their voices. I assume they spend a good amount of their days turning away people in need. Despite these women’s compassion, I cracked. I reached my emotional limit and commenced to sob.
As I wept, I thought back to every crappy clinic I’d visited. I remembered the crackpot doctor who used Google to answer my routine questions. I recalled the times I’d been ripped off because I couldn’t afford another option. I thought about the number of clinic staff who’d told me that if I only had a child I didn’t want and couldn’t care for I’d be eligible for health insurance through the California Medical Assistance Program (Medi-Cal) — but even that doesn’t include coverage for dental work.
I realized I’d gotten so used to receiving poor treatment that I no longer believed I deserved better care. I wonder how many other uninsured Americans believe the same.
I wonder about the lives of people who have health insurance. I imagine the ease of having a dentist who will make an appointment for me because they fear losing my business or care about my well-being. I consider what it must be like to drive to an air-conditioned dentist’s office without having to wait for a perpetually late bus in the smoggy, summertime heat while being harassed by men on the street. I think about handing over a copayment instead of waiting for the visit’s bill, and carelessly allowing the dentist to address my toothache without fear of how much each piece of gauze will cost me.
I want to say I felt happy for the people for whom going to the dentist is not a time of stress and struggle, but my tears in that moment contained only hatred for them and the entire American medical system.
We often don’t consider the long-term toll — personally and as a country — of what it means to have a nation of people who can’t access adequate health care. In addition to our physical depreciation, new research confirms the negative neurological effects of a life plagued by financial anxiety. Having scientific data to back up my personal experience is oddly comforting yet disconcerting. Mostly, it is evidence of the injustice of poverty.
Tina with her mom.
When the poor are treated as collateral damage in a fight between wealthy, well-insured politicians, people like my mom die. It wasn’t so long ago that she and I were snuggled together on the couch, giggling at the sight of my dad cutting that newspaper into squares. And when I am able to find the humor to commiserate with others like me about the absurdity of our situations, I know my mother lives on through me. She gave me what she could when we had nothing at all.
I still haven’t been able to see a dentist about my toothache, and though I have moments when I fear my mother’s and my fates will be the same, the memories of what my mom gave me drive me to keep fighting for something better than she had — so I do.
Raised fatherless and poor in a Haitian coastal town, Dr. Jean-Gardy Marius studied medicine abroad thanks to the financial assistance of an American missionary. Now he is leading an innovative, grassroots effort to root out cholera and bring communities in Haiti’s rural north to health and self-sufficiency.
It’s easy to hear about what’s going wrong in Haiti. Search the news about the beleaguered Caribbean nation, and the negativity overwhelms. Cynical volunteers decry the country’s hopelessness. Aid organizations put forward flimsy justifications for their failures. Frustrated Haitians wait for foreign governments to make good on the “build back better” promises they made, with much fanfare, three years earlier, after an earthquake devastated the country. Today, over 350,000 people continue to live in shelters that were intended to be temporary. The ongoing cholera epidemic has claimed more than 8,000 lives, and malnutrition and famine plague the country.
It is not just that Haiti lacks homes to house its homeless, medicines to treat its sick, and food to feed its hungry. Over the decades, the country has been drained of its human talent, too. There are only four doctors, nurses, and midwives in the country for every 10,000 people, and most of them are located in Port-au-Prince, Haiti’s densely populated capital. The dearth of trained professionals contributes to some heartbreaking health statistics: seventy out of every 1,000 children in Haiti die before their fifth birthday, and 350 out of 100,000 mothers die in childbirth.
It is against this national backdrop of despair that local stories of Haitian resourcefulness and resolution stand out. Even in some of the country’s most impoverished areas, there are people like Jean-Gardy Marius, a Haitian doctor leading an innovative, grassroots effort to root out cholera and bring communities in Haiti’s rural north to health and self-sufficiency.
Photo courtesy of OSAPO
Marius and his humanitarian group OSAPO have worked over the past six years to bring health services to the people of Rousseau, a poor rural community about sixty miles north of Port-au-Prince. When the earthquake struck and cholera spread quickly through tainted water supplies, OSAPO responded by putting up tents to house infected patients, distributing water purification tablets and chlorine, and creating hydration stations for ill people making their way to the hospital — ultimately saving the lives of thousands. OSAPO is now partnering with international aid organizations Oxfam and UNICEF in the country’s north to stem the spread of cholera during Haiti’s hurricane season.
But OSAPO’s efforts go beyond emergency care — and even medical treatment. Marius, who grew up in extreme poverty in a western coastal town, believes that groups like his can provide Haiti’s rural areas with the basic knowledge and resources they need to grow successfully on their own. “Our vision at OSAPO is to improve living conditions,” says Marius, forty-three, whom I interviewed over the phone while he was in Lincoln, Nebraska, in June. “To do that, we have to come up with a good primary health care system. For me, this means education for adults and kids, access to latrines, and healthy drinking water — all the things human beings need to survive.”
After all, the roots of Haiti’s current health crisis go far beyond the 2010 earthquake. The country’s deep and pernicious inequalities have existed since its days as a slave colony, the first one where the slaves revolted and threw off the yoke of colonialism two centuries ago — only to be beset by forced reparations to France, American occupation, and international trade embargoes that stunted its growth from early on. Since then, through brutal dictatorships and corrupt democracies alike, Haiti has struggled to grow its economy in any sustainable fashion, leading to a vicious circle of privation and poor health.
With Haiti’s entrenched poverty in mind, OSAPO has adopted a holistic approach to health care. The group does more than run a health clinic in Rousseau. OSAPO’s staff have trained and deployed health educators into the community to teach people about sanitation, immunization, and family planning. They have dug latrines for 360 families and constructed wells to provide clean drinking water for 2,500 more. They have trained midwives to recognize signs that a particular childbirth might require medical intervention, so that women who live hours away from OSAPO’s clinic will arrive in time to save the mother and child if complications arise.
Photo courtesy of OSAPO
The organization’s focus is on helping people to help themselves. At OSAPO’s clinic, patients are charged nominal fees for each service. The fees, Marius says, are about teaching the community about self-reliance and accountability, while also avoiding the corruption that plagues other clinics. Likewise, instead of handing out food, OSAPO’s nutrition program provides seeds and chickens along with agricultural assistance and educational workshops. “You have to put people back to work,” Marius says. “Agriculture is one of the best solutions to help them economically.”
Marius knows something of self-reliance. The oldest son in a poor family, he never met his father and grew up watching his stepfather abuse his mother. After he stood up to protect her, his stepfather threatened him, and Marius moved in with an uncle.
“I took a bus to his house with hope that he could help me get back into school,” Marius says. “But my uncle used me for household labor.”
At the age of thirteen, Marius ran away from his uncle’s home. For a year, he slept and begged on the streets of Port-au-Prince. Then, a friend brought Marius with him to stay with his family in Pierre Payen, a small village in the northwest. When he was fourteen, he got a job assisting Dr. Victor Binkley, an American surgeon working in Pierre Payen. Through him, Marius met an American missionary who supported him financially when he decided to pursue a medical degree.
After studying medicine in the Dominican Republic and Germany, Marius decided — unlike many of his Haitian peers — to return to his country to work as a doctor.
Photo courtesy of OSAPO
In 2007, he founded OSAPO, or the Oganizasyon Sante Popilè (Popular Health Organization). After a year of working out of a mobile clinic, OSAPO built a permanent health-care center in Rousseau. Today, OSAPO has a staff of five doctors, nine nurses, and one agronomist; last year, it served roughly 52,000 clients.
OSAPO’s model of charging small fees for its services makes sense even in impoverished communities, says Dr. Kim Coleman, a radiologist from Lincoln, Nebraska, who has been to Haiti five times as a visiting doctor at OSAPO’s clinic. She points out that international aid organizations that step in to provide free services can unwittingly create “beggar economies” that undercut local organizations. “The buy-in from patients is so important,” Coleman says, “You can see the damage done by giving handouts. [Marius’s approach] is better for the people, and makes for better compliance.”
Whether foreign aid creates perverse incentives is a major point of controversy in the development world. In recent years, prominent economists such as Jeffrey Sachs and William Easterly have taken opposing views of its effectiveness, while social entrepreneurs ranging from Paul Polak to Muhammad Yunus have argued — to varying degrees — for more market-driven solutions to the problems of poor nations. Perhaps nowhere else is that debate more relevant than in Haiti, which is believed to have more aid groups per capita than any other country except India — as many as 10,000, according to a 2006 report from the World Bank. (During the rule of Haitian dictator Jean-Claude “Baby Doc” Duvalier, foreign governments sought to sidestep the corrupt regime — notorious for funneling aid into Duvalier’s personal coffers — by sending their funds to NGOs instead.)
Since the 2010 earthquake, ninety percent of the six billion dollars disbursed to Haiti has been given to international NGOs and private contractors, while less than half a percent has gone to Haitian businesses and locally run organizations like OSAPO. As the group’s partnership with Oxfam and UNICEF makes clear, the two approaches are not necessarily mutually exclusive. And yet OSAPO’s supporters argue that its cost-effective, comprehensive, and grassroots approach to development should be scaled up. At the moment, Marius points out, there are not even enough qualified candidates to fill his clinic’s need for trained doctors and nurses. If Haiti’s most educated health-care workers continue to flock to Europe and North America, Haiti will need to keep relying on foreign assistance.
Marius hopes that his example will inspire other Haitian professionals to stay at home and tend to a country that desperately needs their talents. When the aid dries up or the foreign doctors fly off, who will be there to care for the sick?
“I wanted to make something that is strong,” Marius says of his group. And in building that vision, he has made the people of Rousseau stronger.
In this excerpt from her recently published book Generation Roe, pro-choice activist Sarah Erdreich talks with women who had an abortion and discusses the complicated set of emotions they bring to the abortion debate — even decades after the procedure.
By Sarah Erdreich
Generation Roe: Inside the Future of the Pro-Choice Movement By Sarah Erdreich
Seven Stories Press. 272 pages.
When people know you work in the pro-choice movement, the stories come out. All of the sudden, you’re a safe person. You can be trusted to hear personal stories about terminating a pregnancy because you won’t judge or criticize. When you go through life hearing such stories, one thing becomes quite clear to you: all kinds of women have abortions. According to the nonpartisan Guttmacher Institute, one in three American women will have an abortion before the age of forty-five.
Rachel (not her real name) is one of my mother’s oldest friends. I have known her and her husband practically all of my life. But it wasn’t until I told them I was writing a book about reproductive rights that Rachel opened up about her own experience with abortion, back in the mid-seventies.
Several years into her marriage, Rachel became pregnant. She had already had two healthy pregnancies, but this pregnancy didn’t progress normally. Rachel was vague on the details when she recounted her story to me, but she made it clear the abortion was medically necessary.
Had I not been offered that option, I very well could have lost my life.… There will always be doubts if I did right or I did wrong, but the right thing is that people can make the choice. I was fortunate that I had good medical care, and I was able to understand my options. But not everyone has that liberty.
“I’m not the least bit ashamed of what I did,” Rachel added. “In fact, I feel somewhat empowered by the choice because that was my right.” Yet Rachel only agreed to be interviewed if her real name was not used.
The day after I spoke with Rachel, I spent some time with a longtime friend of my father’s family. Toward the end of our visit, she mentioned that she had had an abortion many years earlier. Months later, Vicki (also a pseudonym) told me the whole story.
In the early seventies, Vicki became pregnant. Her husband threatened to leave her unless she had an abortion. They were living in a city that was hundreds of miles from her parents, siblings, and closest friends – and in one of the few states that had liberalized its abortion laws by then. “It was [the state’s] law to first see a psychiatrist,” Vicki said. “I remember I told the psychiatrist that if my husband wasn’t in the picture I would not consider abortion, but I guess obtaining the husband’s approval was routine.”
The entire procedure was covered by Vicki’s health insurance. After it was done, her husband — who, she said, had “badgered” her to get the abortion — called her a murderer. She later divorced him.
Vicki never told her family about her abortion.
My ex-husband is the only one who knows. I wanted to tell my mother, but that wasn’t news I wanted to break in a long-distance telephone call. That was back when long-distance calls meant something.… If I’d had more confidence to trust my feelings, and realized I was capable of supporting and raising a child on my own, I would not have had an abortion.
When I worked for the National Abortion Federation, I heard many women express gratitude that they could legally have an abortion, even as they regretted the particular circumstances — an unstable relationship, economic hardship, age, or a lack of education — that made abortion their best choice. To appreciate the right to make your own decision, even as you deplore the circumstances that led to that decision, is a complicated set of emotions that established pro-choice organizations haven’t always successfully addressed.
Groups like Planned Parenthood, NARAL Pro-Choice America, and the National Abortion Federation generally stick to messages about how common and safe abortion is, but they don’t offer a great deal of in-depth discussion about the range of emotions women may experience after having an abortion. Instead, they offer first-person stories, which overwhelmingly talk about abortion in positive terms. While studies have shown that most women feel relief after their abortions, women who have more ambivalent feelings afterward may not find comfort or support in these stories and messages.
The anti-abortion movement has been incredibly persuasive in its insistence that if a woman has mixed feelings following an abortion, then abortion itself must be unethical. In testimony before Congress in 1981, pro-life advocate and therapist Vincent Rue coined the term “post-abortion syndrome” to refer to an adverse physical or emotional response to abortion. While neither the American Psychological Association nor the American Psychiatric Association recognize post-abortion syndrome as an official diagnosis, the term quickly gained traction in the anti-abortion community.
In 1987, Ronald Reagan asked his surgeon general, C. Everett Koop, to write a report about the effects of abortion on women. An avowed opponent of abortion, Koop believed that the procedure traumatized women. He had even coauthored a book, Whatever Happened tothe Human Race, which discussed post-abortion trauma. Even so, he was reluctant to do as Reagan asked. Koop was careful to distinguish between his personal beliefs and scientific evidence, and he refused to let ideology pressure him into taking a stance that the available evidence did not support. Answering Reagan in a January 1989 letter, Koop wrote that he could not conclude one way or another whether abortion was harmful to women.
Koop’s position shocked and incensed his fellow conservatives. President George H. W. Bush declined to appoint him secretary of health and human services in the new administration, and Koop left office one month before the end of his second term as surgeon general.
In 1988, the American Psychological Association commissioned a study to review the research on the psychological effects of abortion. After a survey of over two hundred studies, a panel of six experts found that only nineteen or twenty met what they considered reliable scientific standards. Based on those studies, the panel concluded that “legal abortion of an unwanted pregnancy in the first trimester does not pose a psychological hazard for most women.”
While some women did experience distress, they were in the minority. One study found that “seventy-six percent of women [who had a first-trimester abortion] reported feeling relief two weeks after an abortion, and only seventeen percent reported feeling guilt.”
It is important to note that women seeking later abortions reported more distress after their abortion, as did women who had difficulty making their decisions. While eighty-eight percent of abortions are performed within the first twelve weeks of pregnancy, women who have the procedure done in the second or third trimester overwhelmingly say that the timing was due to a delay in making the necessary arrangements — including raising money and securing an appointment. Fetal abnormality is another reason: many birth defects that are incompatible with life are not discovered until the fourth or fifth month of pregnancy, or even later.
My college years were shaped by the experiences of several close friends who chose to have an abortion following unplanned pregnancies. I learned from their situations that no matter how deeply pro-choice someone might be, it is still normal to have mixed feelings about having an abortion.
“I would never fault a woman who had an abortion for not wanting to share that with other people, because it’s too difficult,” Shannon Connolly, a medical student at the University of Southern California, told me. “But I hope they would be able to. Until abortion is normalized and people are able to say it’s just another part of health care, we won’t be able to talk about it in a meaningful way.”
Sarah Erdreich is a women’s health advocate, writer, and pro-choice activist. Her work has appeared in On The Issues, Lilith, Feminists For Choice, and RH Reality Check.
This excerpt has been slightly edited to adhere to In The Fray‘s style.
This month Americans are celebrating two historic victories for sexual rights handed down by the Supreme Court: the eradication of the federal Defense of Marriage Act and the weakening of a law that required groups fighting AIDS to make an “antiprostitution pledge.”
“The federal statute is invalid, for no legitimate purpose overcomes the purpose and effect to disparage and to injure those whom the State, by its marriage laws, sought to protect in personhood and dignity,” wrote Justice Anthony Kennedy, on behalf of the court’s majority. “By seeking to displace this protection and treating those persons as living in marriages less respected than others, the federal statute is in violation of the Fifth Amendment.”
Although the court’s decision continues to allow individual states to not recognize same-sex marriages performed elsewhere, it does put an end to same-sex unions being “treated as second-class marriage.” It also forces the federal government to provide the immigration benefits of marriage to same-sex couples, thus helping along congressional negotiations over immigration reform that had stumbled over Republican opposition to extending such benefits in the legislation.
Today is the forty-fourth anniversary of the Stonewall riots, which launched the LGBT rights movement in the United States. The Supreme Court’s decision is another landmark for the movement, and yet it also highlights how much farther the country has to go on the path to full equality. Fifteen countries have passed laws permitting same-sex marriage. A dozen more have such legislation pending. And even in some countries where marriage equality continues to face strong opposition — such as Australia, Ireland, Israel, and Colombia — antidiscrimination laws have already been passed that grant LGBT people the right to civil unions and adoption. As for America? Thirteen states down, thirty-seven to go.
The Antiprostitution Pledge
As part of the President’s Emergency Plan for AIDS Relief (PEPFAR) that Congress enacted in 2003, NGOs that received federal funds to fight AIDS internationally were required to sign a statement publicly opposing sex work. Last week, a 6-2 Supreme Court majority struck down the “antiprostitution pledge,” ruling that it violated the First Amendment.
However, the decision affects only US-based organizations. Foreign NGOs who receive US funding can still be required to make the antiprostitution pledge. “The implication for foreign NGOs remains murky,” Chi Mgbako, a professor at Fordham Law School, told the Nation. “Many current and potential recipients of US global AIDS funding are foreign NGOs.”
The antiprostitution pledge has forced organizations to make a difficult decision: denounce the communities they serve, or lose vital funding for lifesaving HIV/AIDS programs. Increasing condom use among sex workers requires demonstrations of correct use, training on negotiating with clients, and collective action among sex workers — all of which could be considered under the policy as “promoting prostitution.”
On the other hand, publicly opposing sex work makes it harder to establish the trust needed to provide services to hard-to-reach men and women. Sex workers are one of the groups most at risk of HIV infection, and yet stigma and discrimination drive them away from the kinds of health education and services that could lower that risk. “At first when we went to [Lima’s] red-light district, people wouldn’t talk to us,” said a health educator at INPPARES, a group that provides sexual and reproductive health services in Peru (disclosure: INPPARES is a member of the International Planned Parenthood Federation/Western Hemisphere Region, where I work). “They’d grab a bunch of condoms and run away.”
Red-light districts also serve as a safe haven for LGBT individuals, where men and women — especially those from rural areas — can freely express their gender and sexual identities. “Many of the clients we work with live as men in the jungle during the week and as women in Lima on the weekends,” said Dr. Daniel Aspicuelta, the executive director of INPPARES.
By hindering NGOs in their fight against HIV/AIDS, the antiprostitution pledge has endangered the lives of sex workers, their clients, and their families. The Supreme Court’s decision has gutted one part of this misguided policy, but it needs to be fully repealed so that groups like INPPARES can do their job.
This post is based on posts on DOMA and the antiprostitution pledge that appeared in the blog of the International Planned Parenthood Federation/Western Hemisphere Region, where I work.
Update, June 29, 2013: This post was revised for length and clarity, and to add disclosures.
He used to make counterfeit credit cards. Now Mansfield Frazier has embarked on an even more audacious project: launching a commercial vineyard in the middle of a poor, inner-city Cleveland neighborhood.
Story and photos by Karen Schaefer
The Vineyards of Chateau Hough, a new winery launched by ex-convict and entrepreneur Mansfield Frazier in one of downtown Cleveland’s poorest neighborhoods. Frazier has ambitious plans for urban farming in Hough: his next project is tearing down the Victorian house alongside his vineyard so that he can build a cellar greenhouse for growing shiitake mushrooms.
A garden hose snakes across the intersection at Hough Avenue and East Sixty-Sixth Street, in a poor urban neighborhood about a mile east of downtown Cleveland. One end is clamped to a city fire hydrant. On the other end, a gaunt man with a weathered face delivers a steady spray of water to the roots of a grapevine.
Around him, another half-dozen workers, dressed in T-shirts and jeans, are hoeing, clipping, and tying up the tender young grapevines of nearly three hundred plants, stretching wires between sturdy wooden posts to trestle the vines. Most of these workers are members of a nearby halfway house, performing court-imposed community service.
Once a deserted lot, the field where they work now boasts three quarters of an acre of prime Cleveland farmland. On one side is a derelict commercial building, partially obscured by weedy trees. On the other side, paint peels from the wooden siding of a boarded-up, white Victorian house.
Welcome to the Vineyards of Chateau Hough.
In the 1960s, the predominantly black neighborhood of Hough was the scene of Cleveland’s race riots, which left four dead and the city burning. For decades, the neighborhood was in decline. The area still has high crime figures and an average income well below the poverty line. Three years ago the corner lot was an overgrown eyesore, made vacant by the demolition of an apartment building abandoned in bankruptcy.
Then local entrepreneur Mansfield Frazier took over the land. At sixty-nine, Frazier is a stout man, whose salt-and-pepper beard skims the broad planes of his smiling face. He is self-educated, a Cleveland native, and a former convict (he prefers the term “formerly incarcerated”). And he is the visionary behind Chateau Hough, a vineyard in the inner city.
His personal story has traced much the same trajectory as downtown Cleveland’s over the past few decades: working-class life disrupted by a descent into lawlessness and poverty, followed by a slow recovery and reorientation toward new, less conventional livelihoods. Frazier grew up about a mile from Hough. He got married at seventeen (much too young, he admits). After high school he got a job with the local electric company. He aced the entrance exam, only to be put to work cleaning toilets. “I worked my way up to be the top welder on the steam line,” says Frazier, “but they would never promote me. They wanted me to train other guys less qualified, to promote past me. And it got very aggravating after a while. I was about to go postal.”
Mansfield Frazier.
After the 1966 race riots tore apart the area, Frazier left Cleveland and began a twenty-nine-year career in counterfeiting. “I manufactured what are called counterfeit access devices, which are credit cards. And I did that all over the country,” says Frazier. “I didn’t mean to be a criminal, I meant to be an outlaw. There’s a difference, you know. Outlaws live outside the law. I didn’t have much respect for American law, because it wasn’t treating people fairly.”
The authorities failed to see the distinction. Frazier says he was never caught, but he was turned in more than once by fellow criminals and served several sentences in various prisons. But in 1992, his life changed while he was working in a prison library. “I was a tutor in math and English and I was reading an article by William Raspberry,” says Frazier, referring to the Pulitzer Prize-winning Washington Post columnist (Raspberry, who wrote about social issues such as race and poverty, died in July). “And I thought he was alright, but he was speaking from wealth — he’d never lived in the projects. So the other clerk said, ‘You think you can write something better?’ And I said, ‘Well, yeah!’ So on a dare, I started writing.”
While in jail, Frazier wrote and published From Behind the Wall (Paragon House, 1998), a commentary on crime, race, and the underclass. The book came out just a few days before his release. Frazier says that’s when the prison psychologist asked him a question: once he got out, was he going to go back to counterfeiting “and make everything in that book a goddamn lie”?
“That stopped me in my tracks,” says Frazier. “I felt like I’d been hit by a two-by-four.”
Frazier decided to see if he could make a success at something other than crime. After his release, he spent some time helping to build houses. Then he launched into his career as a writer. He got a job working for Cleveland’s black newspaper, the Call & Post, and later moved to the City News. He started Reentry Advocate, a bimonthly magazine that now appears in state and federal prisons in twenty states across the nation. These days, his essays on politics and race appear frequently in the Daily Beast, and he also writes a column for a local online magazine, CoolCleveland.com.
Thomas Mulready, publisher of CoolCleveland.com, admires Frazier for his fearlessness. “He’s not afraid to tackle taboo subjects,” Mulready says. “He says things other people aren’t saying.” In a recent commentary on the site, Frazier proposed that Jerry Sandusky, the former Penn State assistant football coach who was convicted of child sexual abuse, should commit suicide.
“I’m a provocateur,” Frazier admits. “I take contrarian points of view. And my background gives me a unique perspective that a lot of people might not have.” Comments about Frazier’s essays show up in almost every issue, Mulready says. “People do disagree with him. But he’s unusual — he often comes back and corrects himself and evolves his position.”
But after years in jail, just writing about social ills wasn’t enough for Frazier. He wanted to do something more tangible to change his community — to help “recreate the black middle class,” in his words. When he got out of prison, Frazier settled down in Hough. He built his own house there and stocked it with vegetable beds, a grapevine, and nut trees. Then he began work on another of his ideas.
An Oasis in a Food Desert
Frazier thumbs through a copy of his magazine Reentry Advocate, which seeks to keep ex-convicts from landing back in prison. After years in prison for counterfeiting credit cards, Frazier became a successful journalist and is now embarking on a new career as an urban farmer.
Across the Rust Belt in recent years, in the empty lots of cities like Cleveland and Pittsburgh, Youngstown and Detroit, urban gardens have been sprouting like spring mushrooms. Generally speaking, urban agriculture is nothing new. In her book Food and the City: Urban Agriculture and the New Food Revolution, journalist Jennifer Cockrall-King points out that urban gardens flourished during World War II: at one point, 40 percent of the nation’s vegetables were grown in these “victory gardens.” (In comparison, local foods expert Brad Masi estimates that today’s urban gardens in greater Cleveland produce about 1 to 2 percent of local food consumption; in cities like Chicago, it may be as high as 5 percent.)
What is perhaps different about today’s urban farms is the focus on reclaiming tracts of land in blighted downtown neighborhoods and planting viable businesses on them. And while the movement is still small, a number of trends in recent years have converged to support it. Against a backdrop of growing interest in climate change and pesticide-free produce, books such as The Omnivore’s Dilemma and documentaries such as Food Inc. have extolled the environmental virtues of locally grown, small-scale agriculture. Urban farming projects have gained national exposure with the success of pioneers like Will Allen, a former professional basketball player and MacArthur “genius grant” recipient who heads one of the country’s largest urban agriculture programs in Milwaukee. Meanwhile, the mortgage crisis that set in motion the Great Recession five years ago has brought about an abundance of available land, as abandoned homes and cratering real estate values have made it affordable to farm again on entire city blocks.
Mansfield Frazier was one local entrepreneur who saw an opening. In 2009, as his city was still reeling from the recession, he applied for an initial $18,000 grant from Reimagining Cleveland, a citywide program designed to support sustainability projects that rebuild neighborhoods. Frazier’s idea was to start a farm on an abandoned city lot. It was not just about making money, he says, but about providing food alternatives in a low-income neighborhood with plenty of fast food, but few healthy options — what experts call a “food desert.”
“What you see young mothers putting in their grocery carts is appalling,” says Frazier. “You’ve got to make healthy choices. You can’t raise kids off of Twinkies and that sugary fruit punch.”
A vineyard was the first stage of Frazier’s plans for his nonprofit farming venture. He admits he didn’t know much about wine when he started (“I’m an expert — at taking the cork out of the bottle”). But Frazier won over his skeptics on the grant committee with his personality and passion, and over the past three years he has studied the art of winemaking intensively through his collaborations with local experts, learning enough to start advising other would-be vintners in the city. “Can’t be that hard, it’s the world’s second-oldest profession,” Frazier jokes. “Grapevines have been around forever. The great thing is, you can screw them up and they still come back.”
Frazier shows one of his workers — also a former inmate — how to tie up some grapevines. Many of the vineyard’s workers are ex-offenders from a nearby halfway house who are performing court-ordered community service.
Neighborhood Progress, a Cleveland nonprofit that funnels federal dollars into local urban agriculture projects, boasts of Frazier’s vineyard as one of their biggest success stories. “His vision is huge — and it’s long-term,” says Lilah Zautner, the organization’s program manager. “He practices what he preaches, he walks the walk. For him to say ‘I want to put a winery and a vineyard in the middle of the inner city in the Hough neighborhood’ is an amazing vision. But also not just to have that vision, but to systematically make that happen.”
The grant from Reimagining Cleveland provided Frazier with the start-up capital for his farm, but local government has also helped him build that: as part of its land-bank program, the city of Cleveland is letting him use the lot virtually for free, so long as he pays the property taxes. Since his business is nonprofit, donations provide the rest of his funding, and local volunteers help out in the fields. And thanks to an agreement with a nearby halfway house, most of the vineyard workers are ex-offenders performing unpaid community service.
“It gives me a chance to mentor,” Frazier says. “We talk when we’re working. Guys say, ‘I’m going to get out, going to get me a dope bag.’ And I say, ‘That didn’t work too well last time. Maybe you want to think about doing something else.’”
Now that the winery is in business, Frazier is moving ahead with plans to expand his urban farm. “That building we intend to do fish-farming in,” he says, pointing at the decaying commercial building next to his lot. “The county wants to give me that building also. They don’t own it, but they’ll take it from the owner; it’s a blight. So we’ll do them a favor and save them from the taxes.” Likewise, Frazier is paying off someone else’s $1,600 tax bill in exchange for the sagging Victorian house on the other end of his vineyard, whose basement he plans to convert into a bio-cellar, a semi-subterranean greenhouse that will be covered with a twenty-foot-high roof of plexiglass. There he’ll grow shiitake mushrooms for local restaurants (they’re selling now for $20 a pound, he notes). Across the street on another vacant property, Frazier sees a vegetable garden whose produce will go to area food banks.
In Hough, the supply is certainly there to meet the demand. Over the last decade there has been some reinvestment in new condominiums and private housing, but much of the neighborhood is still in disrepair, with land bank-owned boarded-up houses and vacant lots. (Overall, Cleveland has 1,200 acres of land — almost 10,000 city lots — available for projects like Frazier’s.)
Just having an urban farm nearby can shape the ways that people in the neighborhood look at their food, Frazier says. “The goal is to train kids and let them see how crops grow, and you can change their eating habits. I think that’s critically important. We are a very unhealthy nation.” And the presence of a growing, locally owned business in Hough will make the community healthier in other ways, too. Frazier sees urban agriculture jobs as a good fit for former inmates reentering the workforce — and as a productive outlet for young people as well, “to keep them off the streets and out of prison.”
Workers tend to the vineyard’s grapevines. Frazier plans to lease the abandoned commercial building in the background from Cleveland’s land bank so that he can convert it into a facility for fish farming.
That’s what Frazier means when he talks — with his characteristically heady ambition — about “recreating the black middle class” in Hough. The neighborhood doesn’t need saviors; it needs investors to tap the potential that’s already there — in the soil, and in the people. “I don’t think the neighborhood is in that much need of redemption,” Frazier notes. “I don’t think the neighborhood is bad.”
This fall, Frazier harvested his first crop. He doesn’t have a winemaking license, so he’s invited amateur vintners in the area to come and use his Traminette and Frontenac grapes. Frazier personally prefers sweeter wines, like Riesling or Moscato. But he says he doesn’t care what kind of wine comes from the grapes. He just hopes that one day locals will be able to buy a bottle of Chateau Hough.
“Everybody wants to see what the ground has wrought,” says Frazier. “And it’s impossible to tell — you can’t predict what the wine’s gonna taste like. And I’m getting curious.
“Who knows? I might even make an award-winning wine.”
Karen Schaefer is a freelance writer in Ohio.
Dear Reader,In The Fray is a nonprofit staffed by volunteers. If you liked this piece, could you please donate $10? If you want to help, you can also:
This not only violates the most basic rights of people living with HIV. It also threatens public health, by making it dangerous for anyone to seek information about HIV prevention or treatment.
—Rebecca Schleifer, of Human Rights Watch (HRW), who addresses issues related to HIV and AIDS.
According to HRW, four Egyptian men were recently detained, shackled to hospital beds, and forcibly tested for HIV; two of the men tested positive. Amnesty International and HRW state that these recent arrests are part of a larger scheme that started last fall, when two men were arrested during a fight in Cairo in October 2007. When one man stated that he was HIV-positive, the men were taken into custody and questioned by the division of the police that investigates questions related to public morality. Both men asserted that they were beaten and forced to undergo rectal examinations that were allegedly intended to prove homosexual behavior. Homosexuality can be indirectly punished in Egypt by charging homosexuals under laws that punish obscenity, prostitution and debauchery.
Abuse and torture by the police is not entirely uncommon in Egypt, an issue which was recently highlighted by camera-phone video footage of police raping a man with a stick.
Just as importantly, treating HIV/AIDS as a crime instead of a severe illness has the potential to dissuade unknown numbers of people from seeking testing and treatment in the country of approximately 75 million.
This is a story about two boys, brothers, born of the same mother, the same father, in the same city, the same hospital, and according to their father, the same bed. These brothers share a love for roughhousing with each other and any comers. You can find them challenging each other in kickball and arguing over which restaurant to share a meal or who can talk the loudest. Together they have moments of mutual satisfaction laced with more than just a few conflicts.
One brother amazed his pediatrician when at eight months he showed up in his office, an overwhelmed mom and dad at his side. "What seems to be the problem?" the standard line given to parents who do not have a clue. "Well, he has been crying all morning, we’ve tried everything, and don’t know what is wrong." "Well, how does he act when he isn’t feeling well?" replies the pediatrician, with a what-a-bunch-of-morons nod of his head. Mom glances at dad, who glances right back. "You mean sick? He’s never been sick." Now the doctor looks up, interest peeked. A never-been-ill eight-month-old? Who knew such a child existed? First-time parents, we thought baby Tylenol was for teething.
The second time around, we learned that weeks-old babies could develop ear infections, that visits to the doctor could become routine, that asthma is a serious thing. Two brothers, one so healthy he dares fate to cast an illness his way, the other tied to nebulizers, graduating to inhalers, plans filed with the nurse’s office, medicine and its accompaniments always kept on hand. Two boys, one healthy, one less so, one breathing clearly, one listening for that little rattle, one confident in his health, one anxious that his medicine might be left behind. One breastfeed, one not.
While health professionals have promoted the benefits of breastfeeding for a number of years, the actual number of women who choose to breastfeed has declined. Common sense would suggest that, as women become aware of the benefits of breastfeeding, at least some increase would emerge. So why the decline?
The Washington Post National Weekly Edition reports on one possibility, government strongarmed by industry. According to their investigation, the infant formula industry hired guns — Clayton Yeutter, agriculture secretary under George H.W. Bush and Joseph Levitt, former director of the Food and Drug Administrations’s Center for Food Safety and Nutrition, which regulates, you guessed it, infant formula — to protect their interests when faced with new, viable research supporting breastfeeding.
As the health and science community completed research indicating that non-breastfeed babies are up to 250 percent more likely to suffer respiratory diseases, the Federal Office on Woman’s Health geared up for a hardhitting ad campaign, featuring a baby bottle nipple attached to the end of an asthmatic inhaler as well as a syringe-topped baby bottle. Images designed to wake up moms to the possible consequences of choosing formula over breast. The promotion of consequences versus benefits is not new to government advertising — think Ad Council campaigns on drunk driving — yet it is an approach, when taken with breast versus bottle feeding, that leaves behind the idea that both are equally healthy and simply a lifestyle choice.
In a "Dear Tommy" letter to former HSS secretary Thompson, Yeutter used mom’s guilt to promote the toning down of the proposed ad campaign. After all, he asked, "Does the U.S. government really want to engage in an ad campaign that will magnify that guilt?" Well, while I can’t speak for all of the moms out there who have chosen to use formula over breastmilk, I can tell you what I think. Yes, I feel guilty that I didn’t endure the painful tearing of my nipples (onionskin comes to mind) when my youngest had difficulty latching. Yes, I feel guilty that I let the fact that I wanted to return to work influence my decision to bottle feed. Yes, I am guilty of putting my own needs over my child’s. I am reminded of that choice every day when I open the kitchen cabinet, the glove compartment of my car, the upstairs closet, and bits of my son’s asthmatic life appear.
I am also frustrated with a government that would promote immediate dollars over the health of its children. Of course encouraging moms to breastfeed means not only damaging the infant formula industry, it means supporting moms in the workplace. It could mean longer paid (what a concept) maternity leave, on-site childcare, or alternative workplace locations. Like a line of tipped dominoes, a hardhitting ad campaign on the consequences of not breastfeeding starts alone, only to knock its universe on its backside.
We use cookies to improve your experience while you navigate through the site. Cookies that are categorized as necessary are stored on your browser, as they are essential for the working of the site’s basic functionality. We also use third-party cookies that help us analyze and understand how you use this site. These cookies will be stored in your browser only with your consent, and you have the option to opt out of using them.
Necessary cookies are essential for the basic functionality and security features of this website. These cookies do not store any personal information.
Any cookies that are not necessary for the website to function and are used to collect user personal data via analytics or other embedded content are termed non-necessary cookies. It is mandatory to procure user consent prior to using these cookies.

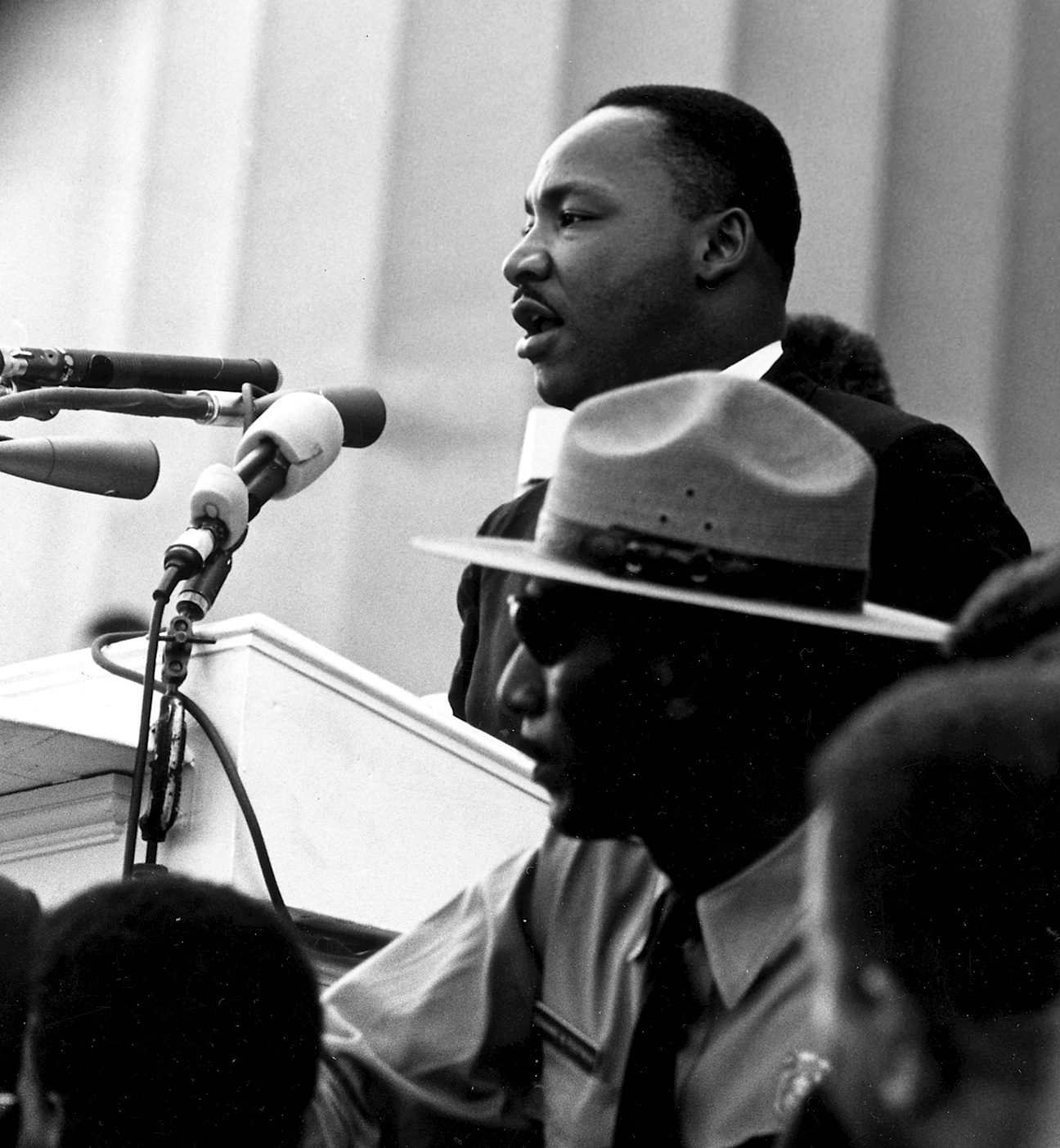



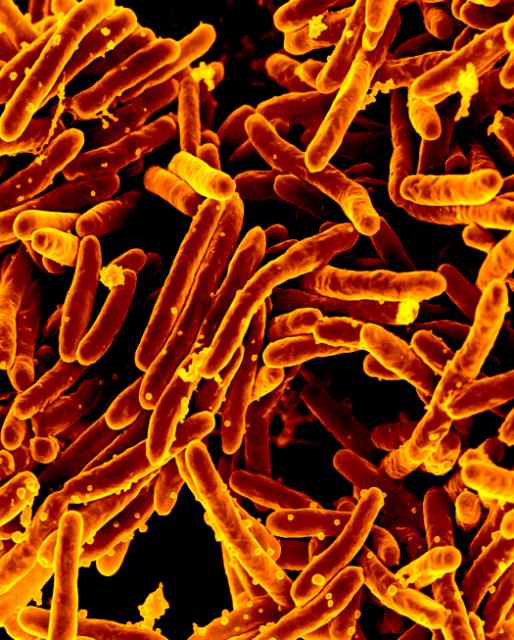
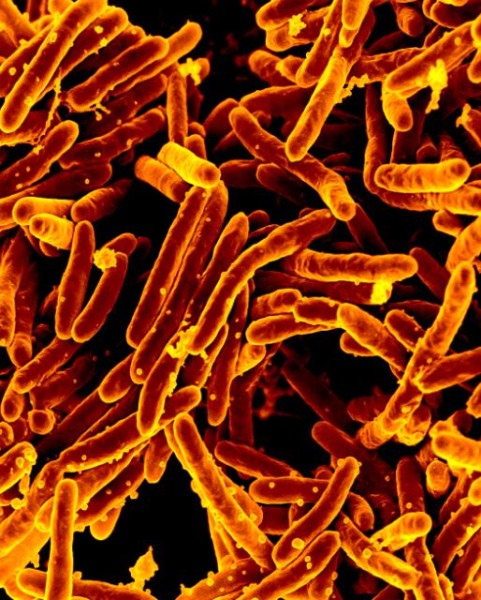


















{kind=link}